An ABM Approach to Addressing the Opioid Crisis: How can we predict the effects of public health intervention on a unique community of pain patients?
Contributors to this project include Allison Young, Georgiy Bobashev, and Jay Rineer.
Check out the Github repoEvery day, more than 130 US adults die from opioid overdoses. Opioid misuse has become a national public health crisis affecting individuals across the country and in our own backyards [1]. In the last 20 years, the number of medication and drug poisoning deaths in North Carolina has increased nearly six-fold, from about 400 deaths in 1999 to more than 2,400 in 2017. North Carolina has taken steps to prevent these deaths, most significantly through the 2017 North Carolina Opioid Action Plan, which focuses on prevention of opioid misuse, reduction of harm, and expansion of connections to care. Just two years after the Action Plan’s launch, opioid dispensing has decreased by 24%, prescriptions for drugs used to treat opioid use disorders has increased by 15%, and opioid use disorder treatment for uninsured and Medicaid beneficiaries has increased by 20% [2].
Despite these advances, the number of opioid related deaths has not declined [3]. To tackle this issue, Allison Young and I partnered with RTI International to answer three questions:
The ultimate goal of this research is to prevent opioid-related deaths, whether in the state of NC or otherwise. This work provides evidence that disparate data sources can be combined to identify potentially effective interventions tailored to specific communities. Our analysis is a preliminary step in a larger investigation, designed to provide proof of concept for a multi-million dollar grant proposal to look more in-depth into these research questions and approaches. With additional resources, research can continue through RTI International or through the NC Department of Health and Human Services.
Agent-based modeling (ABM) has been shown to be an effective approach to examine the effects of opioid interventions. These models simulate the lives of patients prescribed opioids under different proposed policies.
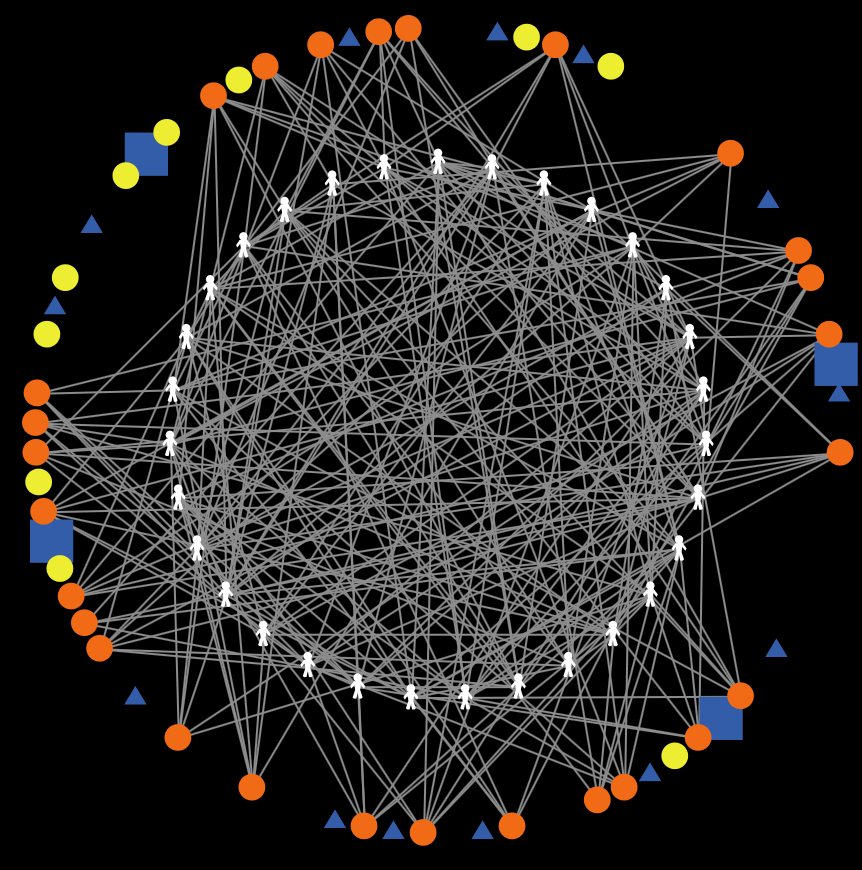
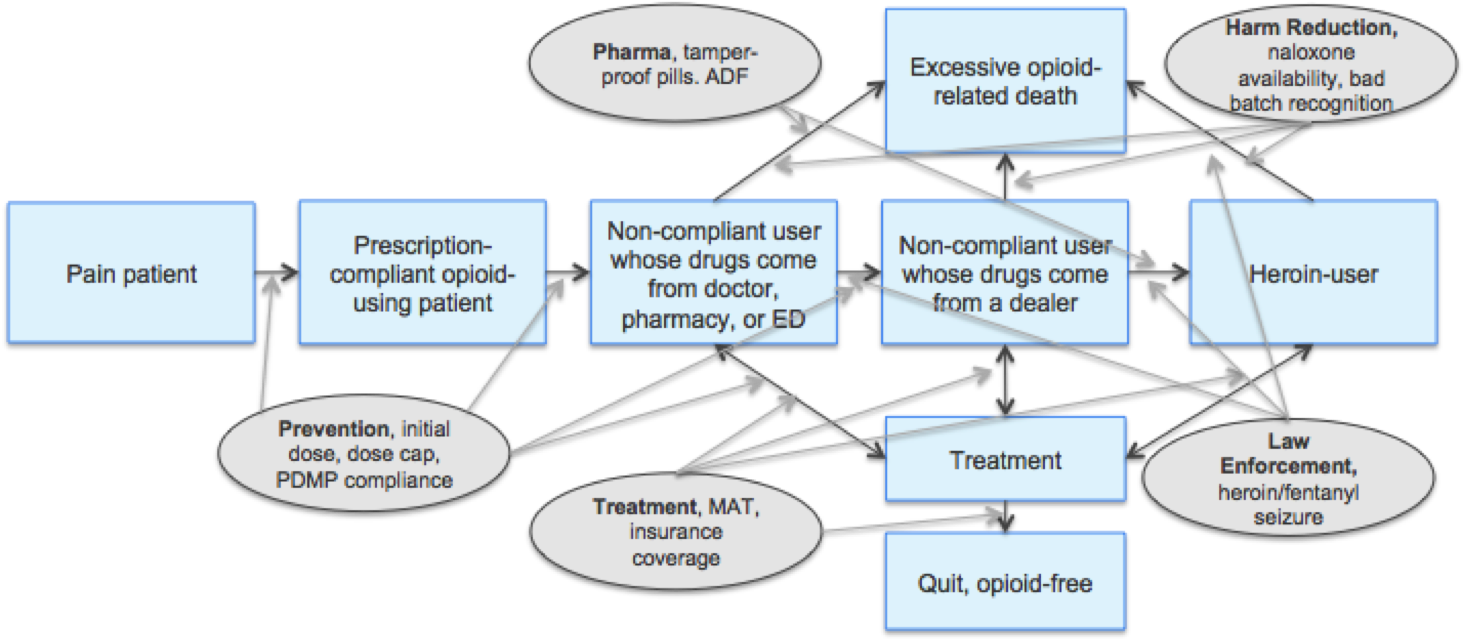
The ABM takes input measurements including the number of agents (such as size of population and number of providers and pharmacies), in addition to local measurements of behavior and available resources (such as naloxone availability and the PDMP compliance rate). The model itself then simulates the lives of drug users by sending each agent through a series of daily actions, determining the actions they take and paths they follow based on probabilities found in literature and research. Agents are connected to one another through their own social networks, simulating a true community. At the end of the allotted time period (in our case 5-years), the model will summarize outcomes as the number of opioid and heroin overdoses, deaths, and patients who are not following recommended medication prescriptions. Policies are ultimately evaluated based on overdose and mortality rates of prescription opioid users and heroin users, as well as on the number of patients who become non-compliant with their prescription and turn to illicit drug use.
Although previous ABM research has shed significant insights into effective methodologies for investigating the opioid crisis, there are many nuances to consider. Previous ABM research has used generic populations; however every community has unique demographics, policies, and capabilities for care. By tailoring our model to a specific population, insights are simple to extrapolate and act on.
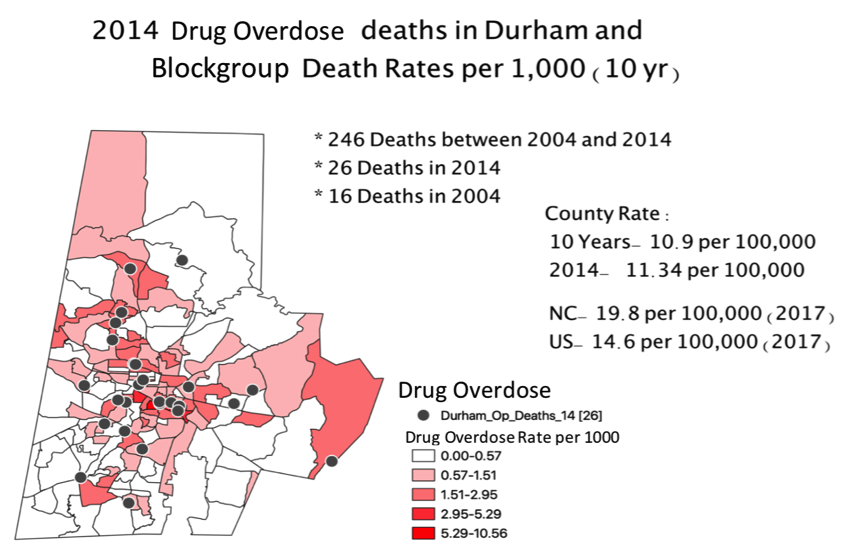
To understand who is dying from the opioid crisis, we first examined where Durham residents are dying from opioid-related causes. This analysis utilized geocoded death records from 2010 to 2016 made available by the NC State Center for Health Statistics (NC SCHS) and RTI. [5, 6, 7, 8] .
A descriptive analysis suggests that Durham rates of opioid and drug overdose deaths mirror trends for the nation as a whole. From 2004-2014, 80% of deaths related to drug overdoses occurred for individuals between the ages of 31 and 60. 63% of opioid overdose deaths were represented by white residents, while the population is only 50% white [9].
From a geographic standpoint, we also see a cluster of deaths near the Lakewood and Golden Belt neighborhoods of downtown Durham. Sparsely populated block groups in Durham are disproportionately high in opioid-related deaths compared to the population of the county. We suspect that many of these deaths occur in public areas such as large parks as opposed to residential areas.
Modeling a community of pain patients is no simple task. Considering the life of just one pain patient involves hundreds of decisions, actions, and outcomes. Incorporating multiple pain patients introduces a tangled web of relationships and interactions. Modeling these communities of pain patients is possible with agent-based models, which effectively simulate the lives of patients prescribed opioids over the course of five years. These models are enormous collections of agents running through identical Markov chains for a fixed period of time.
In order to improve upon previous research, much of our work revolved around tailoring an existing general ABM to the demographics, policies and outcomes of Durham County. This tailoring was accomplished through 1) a review of existing literature and 2) calibration to ensure our model accurately predicted local outcomes.
The results of the literature review informed the parameters of our ABM. This step proved to be a particularly challenging and time intensive process, as local data is often unavailable. Where possible, parameters reflect that of Durham County specifically. Where we could not find local data, national literature was used. When national data was not available, we relied on client estimates. Finally, where we did not find evidence of deviation from the default, variables were left at their original values.
After gaining as much information as possible from literature, we altered additional ABM features in the interest of consistently simulating Durham County outcomes. After much experimentation, we succeeded in replicating Durham outcomes by updating several model features including increasing the probability of overdose, increasing probability of a bad batch of heroin entering the community, and increasing the additional risk of overdose and death by heroin.
In the final stage of our analysis, we used our calibrated ABM model to simulate the effects of a variety of interventions. As previously described, ABM allows us to simulate the effects of inventions on a specific population. Importantly, ABM applies each intervention in systematic fashion allowing us to predict the effects of each intervention at varying levels. A promising intervention would be one that predicts fewer deaths, overdoses, or patients who are non-compliant.
Specifically, we explored the effects of six different interventions: 1) naloxone availability, 2) PDMP compliance, 3) Emergency Department (ED) initial dosage, 4) buprenorphine treatment chance, 5) average prescribing rate, and 6) average ED prescribing rate. We applied each intervention 50 times at five varying degrees. By running so many iterations, our estimates are protected from the effects of any single outlier. We evaluated the effects of these interventions based on five outcome metrics 1) number of opioid overdoses, 2) number of opioid deaths, 3) number of heroin overdoses, 4) number of heroin deaths, 5) number of heroin users.
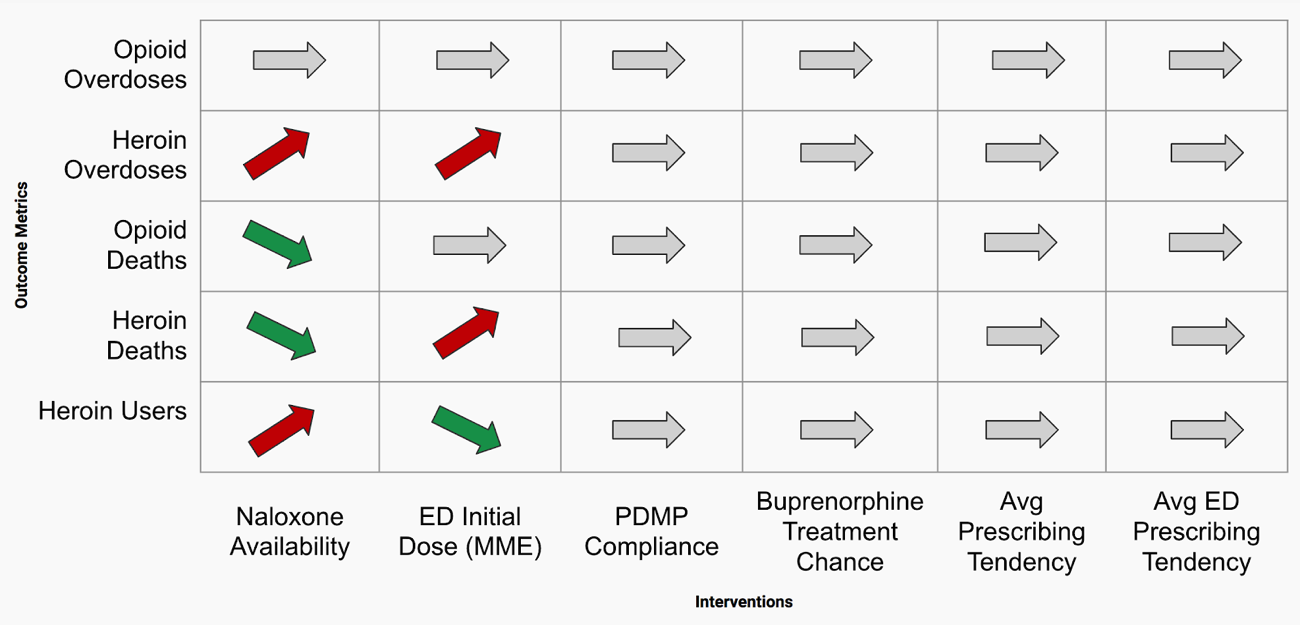
Our results suggest that naloxone availability and ED initial dose have the largest effect on outcomes. According to our findings, increased naloxone availability was associated with increased overdoses but a decreased death rate, while ED initial dosages over 75 MME was associated with increased heroin overdoses and deaths.
Naloxone is an opioid antagonist, meaning that it binds to opioid receptors and can reverse and block the effects of opioids [16]. Naloxone is used to rapidly reverse opioid overdose and ideally prevent death from overdose. Increased availability of naloxone was associated with increased overdoses, but a decreased death rate. We believe that by increasing the probability of receiving naloxone, fewer patients are dying and are remaining in the community. With the increased number of pain patients, the number of overdoses subsequently increases due to the larger sample. This trend seems to also be apparent in both the opioid and the heroin user populations.
Emergency departments (ED) may distribute new opioid prescriptions. Smaller initial doses are thought to decrease the rate at which compliant opioid users become dependent on their prescriptions. Our findings suggest that ED initial dosages over 75 MME are associated with increased heroin overdoses and deaths. This finding supports the hypothesis that increased initial doses lead to patients with high tolerance and desire for opioids. This high tolerance and desire may lead compliant opioid users to seek additional narcotics such as heroin, eventually leading to increased heroin overdoses and death.
Opioid overdose deaths affect both rural and urban populations in Durham equally. However, opioid overdose deaths do appear to be most prevalent in middle-aged white men. Initial exploratory data analyses allude to potential hotspots for overdoses in areas with public parks or areas adjacent to recovery communities. Further quantitative and qualitative research is needed to validate this hypothesis.
Using ABM, we successfully modeled the outcomes of pain patients in Durham. This step should not be understated, as it required combining an extensive body of research into a single model, a task that was thought by many health officials to be impossible. Our ABM is a meaningful step in understanding the complex behaviors and relationships involved in the lives of local chronic opioid and heroin users. This is proof of concept that these data can be combined to provide meaningful insight, with the understanding that these models are just a starting point, as properly parameterizing them, and ensuring they encompass all major effects, requires significant future work.
Our findings suggest that increased naloxone availability and ED initial doses below 75 MME are associated with improved outcomes such as decreased overdoses and death rates. However, interventions such as increased buprenorphine availability and average prescribing rates do not meaningful affect outcomes. This is evidence that policies such as the NC STOP Act may not have their intended effect, or that resulting shifts in behavior may still result in negative outcomes.
Many of the limitations of this analysis could be addressed through qualitative interviews or focus groups with any agent that experiences or touches the lives of opioid drugs. Once these limitations have been addressed, we are confident in prescribing this approach to further public health research across Durham County, North Carolina, and elsewhere.
Want to see more? Read the Full Report Here[1] National Institute on Drug Abuse. (2019, January). Opioid Overdose Crisis.
[2] NCDHHS (2019). North Carolina’s Opioid Action Plan.
[3] National Institute on Drug Abuse. (2020, March). Overdose Death Rates.
[5] SAMSHA (2019a). Buprenorphine Provider Locator.
[6] NCDHHS Safer Syringe Initiative (2019). Syringe Exchange Programs.
[7] NC Dept of Insurance (2019). Operation Medicine Drop.
[8] SAMHSA (2012). Substance Use and Mental Disorders in the Raleigh-Durham-Cary CSA.The NSDUH Report.
[9] NC DPH IVP Branch (2018). North Carolina Poisoning Surveillance Definitions.
[16] National Institute on Drug Abuse. (2020, February). Opioid Overdose Reversal with Naloxone.
An ABM Approach to Addressing the Opioid Crisis: How can we predict the effects of public health intervention on a unique community of pain patients?