An ABM Approach to Addressing the Opioid Crisis: How can we predict the effects of public health intervention on a unique community of pain patients?
With Agent-Based Modeling (ABM), we can predict outcomes for local communities of pain patients. This is an exciting proof of concept suggesting that a similar approach can be applied to other communities to model local health outcomes. An ABM tailored to the Durham, NC pain patient community suggests that increased naloxone availability and decreased emergency department dosages are associated with improved outcomes. Our findings also suggest that interventions such as increased buprenorphine availability and decreased prescribing rates do not meaningful affect outcomes. This is evidence that recent policies may not have their intended effect.
Contributors to this project include Allison Young, Georgiy Bobashev, and Jay Rineer.
Check out the Github repoEvery day, more than 130 US adults die from opioid overdoses. Opioid misuse has become a national public health crisis affecting individuals across the country and in our own backyards [1]. In the last 20 years, the number of medication and drug poisoning deaths in North Carolina has increased nearly six-fold, from about 400 deaths in 1999 to more than 2,400 in 2017. North Carolina has taken steps to prevent these deaths, most significantly through the 2017 North Carolina Opioid Action Plan, which focuses on prevention of opioid misuse, reduction of harm, and expansion of connections to care. Just two years after the Action Plan’s launch, opioid dispensing has decreased by 24%, prescriptions for drugs used to treat opioid use disorders has increased by 15%, and opioid use disorder treatment for uninsured and Medicaid beneficiaries has increased by 20% [2].
Despite these advances, the number of opioid related deaths has not declined [3]. To tackle this issue, Allison Young and I partnered with RTI International to answer three questions:
The ultimate goal of this research is to prevent opioid-related deaths, whether in the state of NC or otherwise. This work provides evidence that disparate data sources can be combined to identify potentially effective interventions tailored to specific communities. Our analysis is a preliminary step in a larger investigation, designed to provide proof of concept for a multi-million dollar grant proposal to look more in-depth into these research questions and approaches. With additional resources, research can continue through RTI International or through the NC Department of Health and Human Services.
Agent-based modeling (ABM) has been shown to be an effective approach to examine the effects of opioid interventions. Bobashev et al. [4] used ABM to predict the effects of opioid interventions on opioid and heroin overdoses and deaths over a five-year period. These models simulate the lives of patients prescribed opioids under different proposed policies. The ABM takes input measurements including the number of agents (such as size of population and number of providers and pharmacies), in addition to local measurements of behavior and available resources (such as naloxone availability and the PDMP compliance rate).
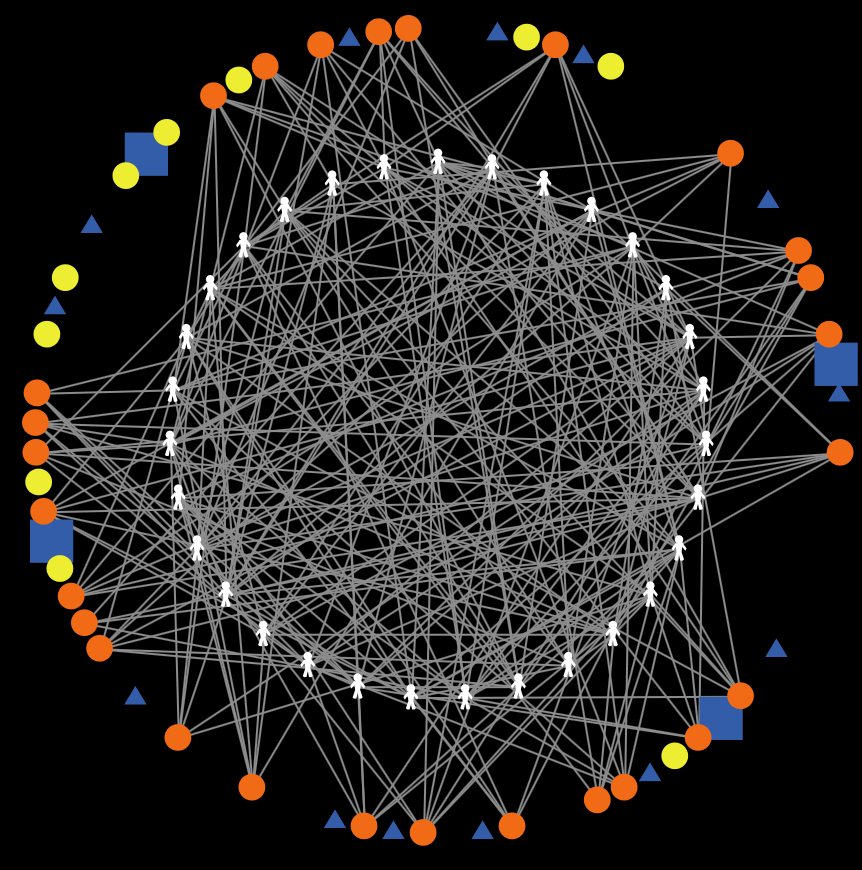
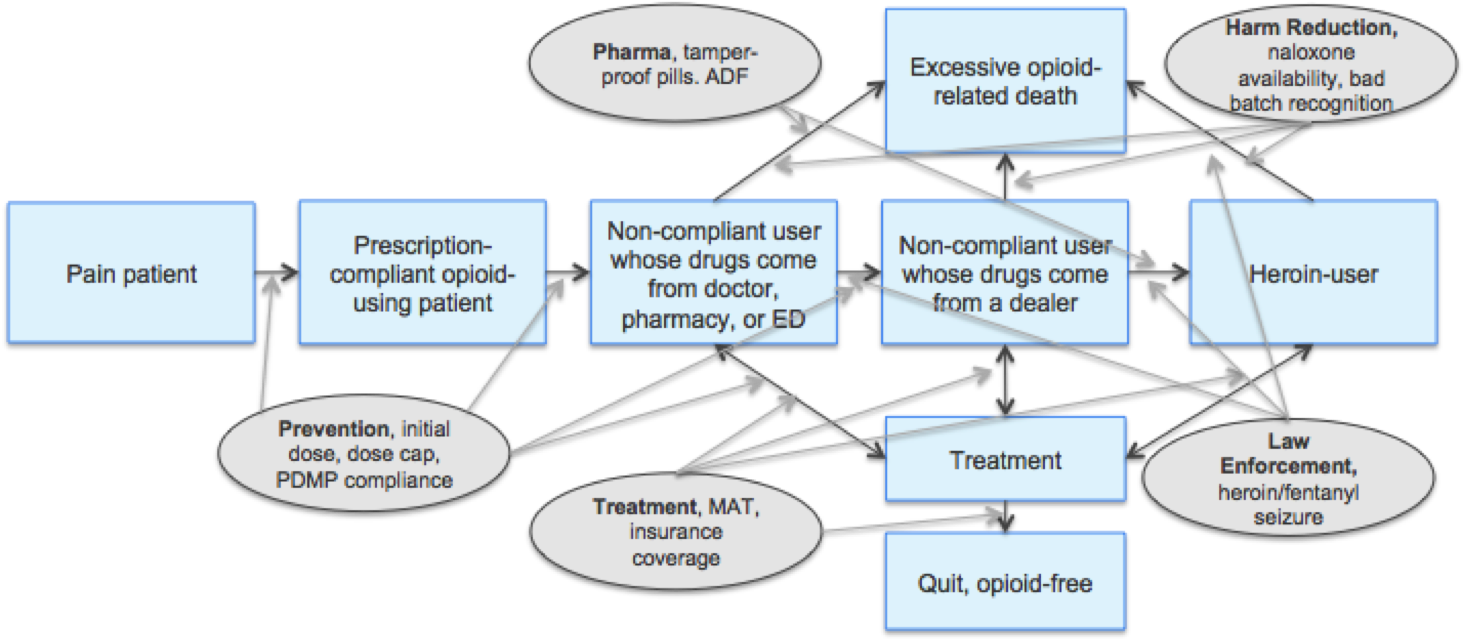
The model itself then simulates the lives of drug users by sending each agent through a series of daily actions, determining the actions they take and paths they follow based on probabilities found in literature and research. Agents are connected to one another through their own social networks, simulating a true community. At the end of the allotted time period (in our case 5-years), the model will summarize outcomes as the number of opioid and heroin overdoses, deaths, and patients who are not following recommended medication prescriptions. Policies are ultimately evaluated based on overdose and mortality rates of prescription opioid users and heroin users, as well as on the number of patients who become non-compliant with their prescription and turn to illicit drug use. This work suggests that ABM can be used to evaluate the effects of various interventions.
Although previous ABM research has shed significant insights into effective methodologies for investigating the opioid crisis, there are many nuances to consider. Previous ABM research has used generic populations; however every community has unique demographics, policies, and capabilities for care. Without tailoring models to specific populations, insights are often hard to extrapolate. What is found to be true in one community is not likely generalizable to another population.
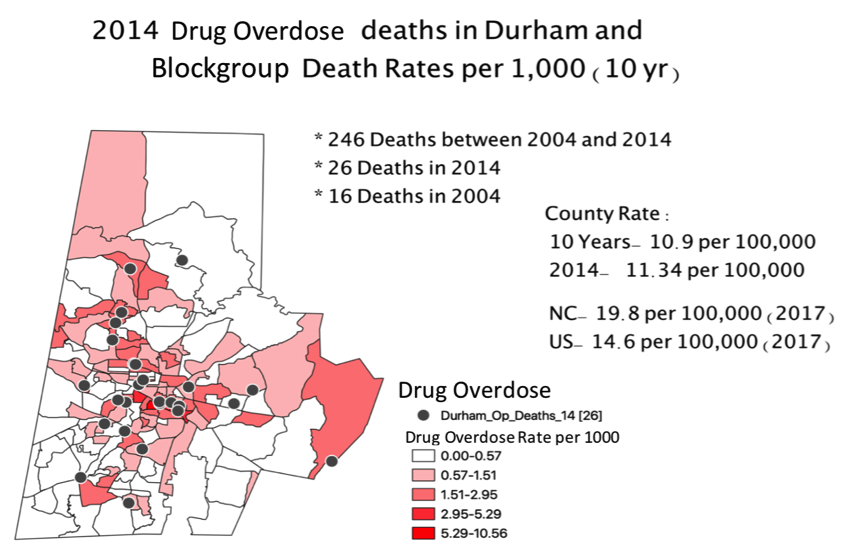
To understand who is dying from the opioid crisis, we first examined where Durham residents are dying from opioid-related causes. This analysis utilized geocoded death records from 2010 to 2016 made available to us by the NC State Center for Health Statistics (NC SCHS) and RTI. Using the case definitions from the NC Department of Public Health Injury Epidemiology and Surveillance Unit Website, cases of opioid-related deaths were identified and further classified as medication or drug poisoning (encompassing all kinds of drug poisoning), opioid poisoning (encompassing all kinds of opioid poisonings, including heroin), and heroin poisoning. We also used publicly available resources to map interventions available for NC residents including locations of providers offering buprenorphine, needle exchange programs, medication drop boxes, and SAMSHA recognized treatment programs [5, 6, 7, 8] .
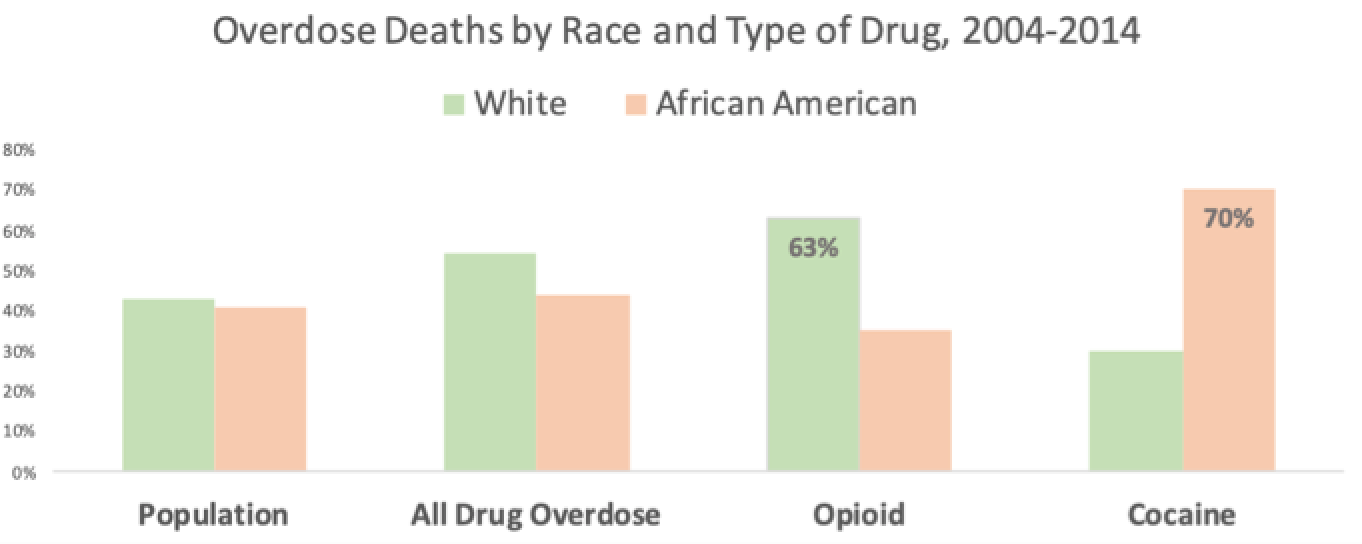
Exploratory data analysis found that Durham rates of opioid and drug overdose deaths mirror trends for the nation as a whole. From 2004-2014, 80% of deaths related to drug overdoses occurred for individuals between the ages of 31 and 60. 63% of opioid overdose deaths were represented by white residents, while 70% of cocaine overdose deaths were represented by African American residents. In both of these cases, the death rates by race are disproportionate to the true Durham population, which was approximately 50% white and 37% African American in 2014 [9]
From this analysis, we can also see a cluster of deaths near the Lakewood and Golden Belt neighborhoods of downtown Durham. Sparsely populated block groups in Durham are disproportionately high in opioid-related deaths compared to the population of the county. We suspect that many of these deaths occur in public areas such as large parks as opposed to residential areas.
An interesting finding from the initial data analysis revealed an unusually high rate of drug overdose deaths in the parking lot of a shopping center off East Lakewood Avenue. Upon further investigation, we discovered this shopping center included a Durham Wellness City location. Durham Wellness City is a community of individuals “embarking on or expanding their recovery” from addiction. This case study is one example of where our work could be strengthened by additional qualitative research.
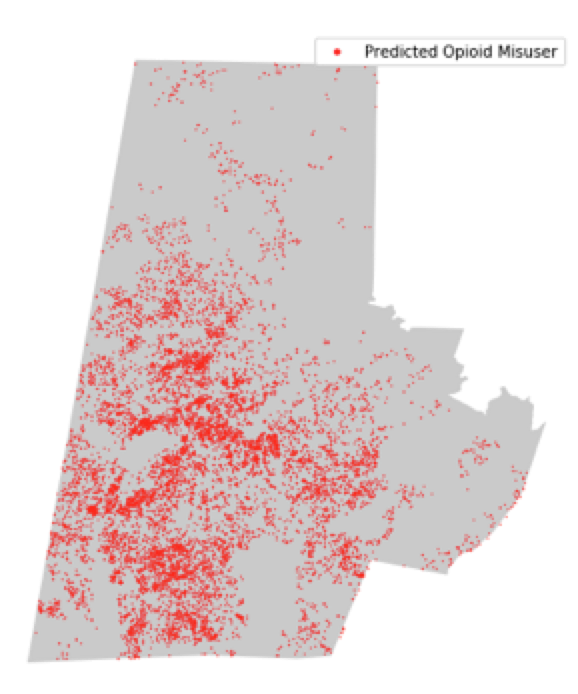
Beyond identifying locations of opioid-related deaths, we attempted to identify hot spots for opioid-misuse residences in Durham County. We utilized synthetic population data and the National Survey of Drug Use and Health (NSDUH) to predict these local opioid-misusing residences.
RTI’s U.S. Synthetic Household Population dataset [10] is a completely synthetic dataset generated from the census and the American Community Survey (ACS) and represents the entire U.S. population. In other words, each individual in this dataset does not represent any real person, however aggregate statistics as small as the blockgroup level are almost identical to aggregate statistics of true population data. With this approach, we are able to protect people’s privacy, circumvent approval processes, as well as incur the benefits of a complete dataset with few outliers.
RTI’s Synthetic Population includes demographic variables such as individual age, race, sex, but does not include opioid misuse or other predictors such educational attainment. In order to augment RTI’s Synthetic Population with these variables we utilized the NSDUH 2018 [11]. Generally, NSDUH provides up-to-date information on tobacco, alcohol, and drug use, mental health, and other health-related issues in the United States. Using NSDUH and logistic regression, we first predicted synthetic individuals’ educational attainment, and subsequently predictions of individual opioid misuse in the past 12 months.
A 75-25 train test split was used to model educational attainment using NSDUH 2018. Predictions of educational attainment on synthetic populations resulted in an overall accuracy of 0.5864. A 75-25 train test split was similarly used to model opioid misuse using NSDUH 2018. Predictions of opioid misuse resulted in an accuracy of 0.959. Although accuracy is high, this merely represents the unbalanced nature of the opioid misuse variable. Only 4.1% of NSDUH respondents report misusing opioids in the past 12 months. Area under the curve (AUC) for our predictions is only .5166. Various techniques were explored to combat this imbalance. Despite these attempts, the AUC remained similarly poor.
Unfortunately, our predictions of opioid misuse are only slightly better than chance. However, this is not entirely surprising given we are merely using demographic variables to predict complex behavior such as opioid misuse. Nevertheless, based on our predictions of opioid misuse in the past 12 months, we classified individuals with the highest predicted probability as “predicted opioid misusers”. The threshold for classification was set to the top 4.1% of predicted values based on the national rate of reported opioid-misuse (NSDUH, 2018). Our map of predicted opioid misuse in Durham County shows varying concentrations of misuse occurring across the county with hot spots located in the center of the county. We can also see the outline of the highways running through the county as a cross in the center of the county. Based on the low accuracy of our predictions, we suspect that any trends are mostly reflective of population density. Future research should focus on improving the accuracy of these predictions to better identify hot spots for opioid misuse. With these improved predictions, a direct comparison between predicted opioid misuse households and mortality records would be valuable. This comparison map may help identify areas where deaths occur outside of the home.
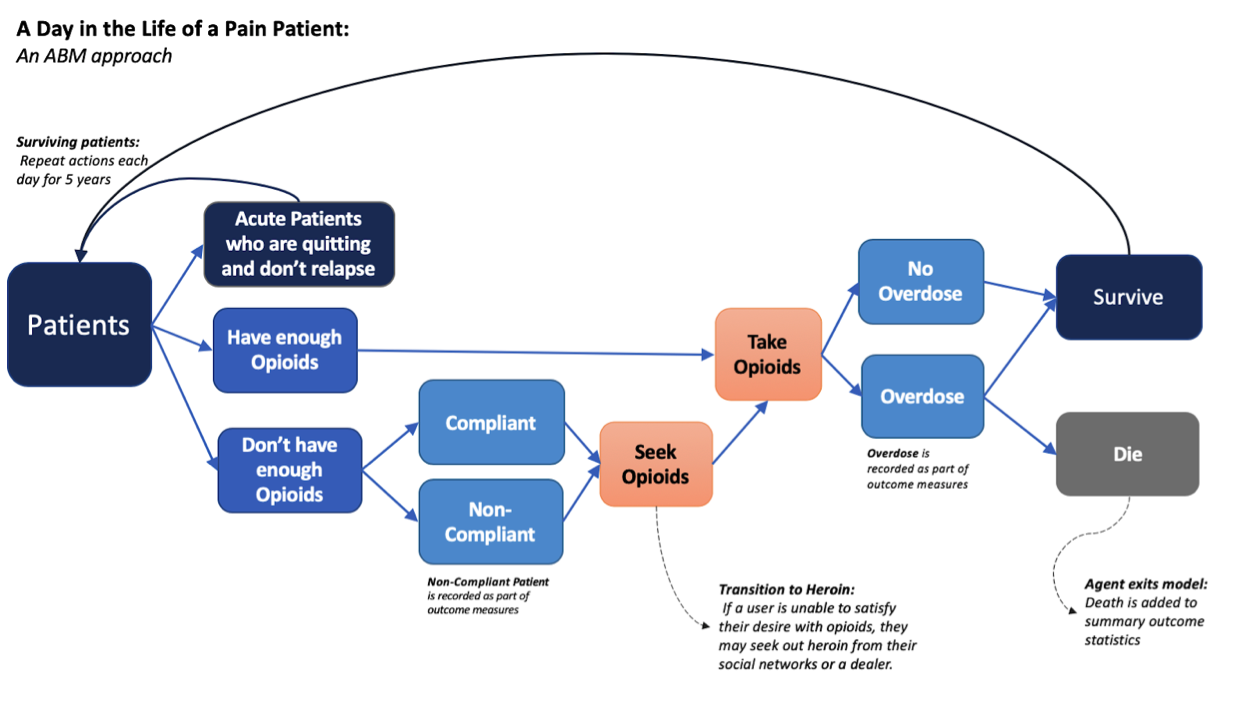
Modeling a community of pain patients is no simple task. Considering the life of just one pain patient involves hundreds of decisions, actions, and outcomes. Incorporating multiple pain patients introduces a tangled web of relationships and interactions. Modeling these communities of pain patients is possible with agent-based models, which effectively simulate the lives of patients prescribed opioids over the course of five years. These models are enormous collections of agents running through identical Markov chains for a fixed period of time.
In order to improve upon previous research, much of our work revolved around tailoring an existing general ABM to the demographics, policies and outcomes of Durham County. This tailoring was accomplished in three steps, 1) review of existing literature 2) addition of new variables and 3) calibration to ensure our model accurately predicted local outcomes.
The first step in tailoring an ABM to Durham County was to conduct a literature review. Results of this review informed the parameters of our ABM. This step proved to be a particularly challenging and time intensive process, as local data is often unavailable. Where possible, parameters reflect that of Durham County specifically. Where we could not find local data, national literature was used. When national data was not available, we relied on client estimates. Finally, where we did not find evidence of deviation from the default, variables were left at their original values.
Beyond updating the current variables, we also included two new variables relating to buprenorphine medication: buprenorphine treatment chance and buprenorphine effectiveness. Buprenorphine is a treatment for opioid addiction that diminishes the effects of physical dependence to opioids, such as withdrawal symptoms and cravings [12]. Buprenorphine can be used in isolation or along with other treatments such as naltrexone. For those that adhere to buprenorphine treatment, 30% did not relapse after the first year of treatment [13].
After gaining as much information as possible from literature, we altered additional ABM features in the interest of consistently simulating Durham County outcomes. After much experimentation, we succeeded in replicating Durham outcomes by updating several model features including increasing the probability of overdose, increasing probability of a bad batch of heroin entering the community, and increasing the additional risk of overdose and death by heroin.
.png)
The probability of overdose is calculated based on the patients current supply of opioids and heroin combined. This calculation is based on previous medical research on opioid doses and overdose rates [14, 15]. However, our findings suggest that this probability should be increased by a factor of approximately 1.7 to better replicate Durham County outcomes. Although a factor of 1.7 may seem large, even in the most extreme cases an individual’s probability of overdosing on any given day never exceeds 0.00047.
There are many potential explanations for this increased probability of overdose. An unlikely explanation being that the population of Durham has a heightened probability of overdose compared to the general population due to biological factors. A more likely explanation being that local community structure has led to the increased probability. Perhaps Durham suffers from a lack of communication about the risks of high dosage opioid and heroin dosages. Yet another explanation involves imperfections in the original research’s generalizability. The studies on which the original formula was based come from medical research examining the effect of varying prescribed opioid dosages. It may be the case that results of this research cannot be extrapolated to noncompliant opioid users. None of these hypotheses are supported or contradicted by our work. Further research should examine explanations for this increased probability of overdose.
Our experimentation led us to believe that three factors directly impact the number of heroin deaths 1) the probability of overdosing on heroin, 2) the probability of dying after overdosing on heroin, and 3) the probability of a bad batch of heroin entering the community. In regards to the first and second of these factors, our ABM predicts that using heroin increases an individuals’ probability of overdosing and dying by a factor of 2.0 and 3.0 respectively. This is due to our client’s belief that using heroin increases the risk of overdose and death beyond that of using opioids. In regards to the third factor, our ABM consistently predicts that over 99% of deaths from heroin are due to using bad batches of heroin as opposed to taking more than an individual’s tolerance. Because of this relationship, the probability of a bad batch of heroin entering the community has a direct impact on the number of heroin overdoses. These three factors alone almost entirely determine the number of predicted heroin deaths.
Unfortunately, we did not find evidence to support any one particular balance of these three factors. Because of this lack of evidence, the current balance between these three factors should be interpreted with caution. These values generate an accurate simulation of Durham County outcomes, but it may very well be the case that another combination of the three values would do the same. Further research should examine the heightened risk of heroin usage over opioid usage as well as the probability of a bad batch of heroin in a community.
In the final stage of our analysis, we used our calibrated ABM model to simulate the effects of a variety of interventions. As previously described, ABM allows us to simulate the effects of inventions on a specific population. Importantly, ABM applies each intervention in systematic fashion allowing us to predict the effects of each intervention at varying levels. A promising intervention would be one that predicts fewer deaths, overdoses or patients who are non-compliant.
Specifically, we explored the effects of six different interventions: 1) naloxone availability, 2) PDMP compliance, 3) ED initial dosage, 4) buprenorphine treatment chance, 5) average prescribing rate, and 6) average ED prescribing rate. We applied each intervention 50 times to the ABM at five varying degrees. By running so many iterations, our estimates are protected from the effects of any single outlier. We evaluated the effects of these interventions based on five outcome metrics 1) number of opioid overdoses, 2) number of opioid deaths, 3) number of heroin overdoses, 4) number of heroin deaths, 5) number of heroin users.
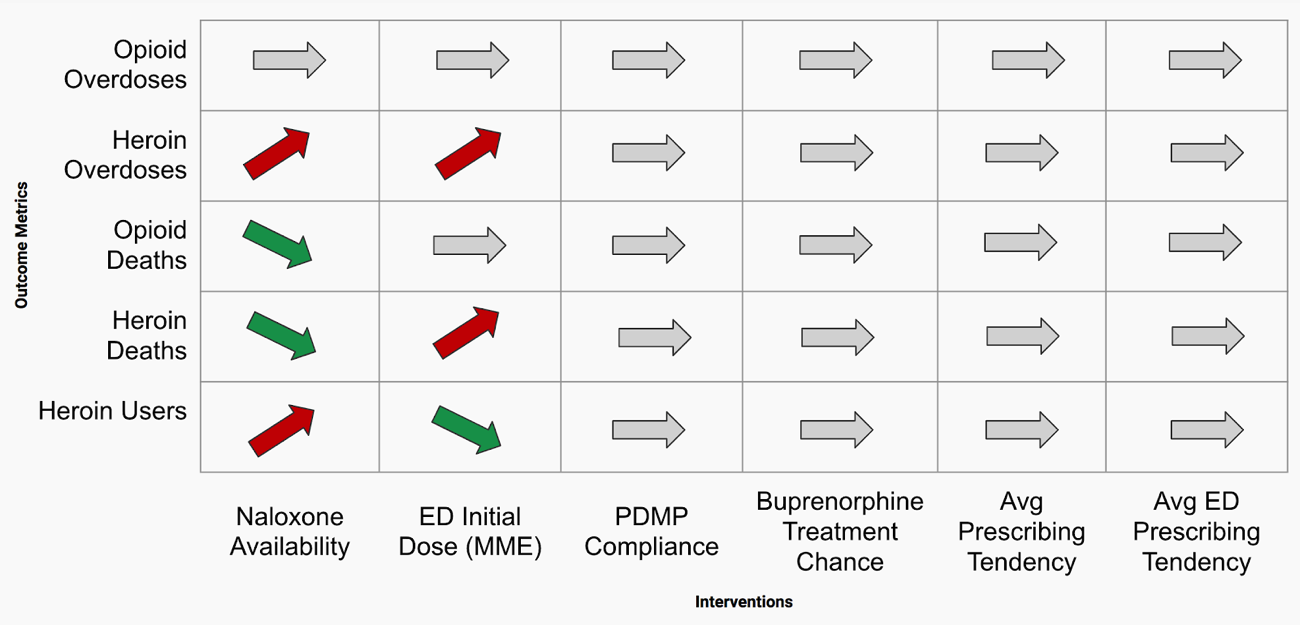
Our results suggest that naloxone availability and ED initial dose have the largest effect on outcomes. According to our findings, increased naloxone availability was associated with increased overdoses but a decreased death rate, while ED initial dosages over 75 MME was associated with increased heroin overdoses and deaths.
Naloxone is an opioid antagonist, meaning that it binds to opioid receptors and can reverse and block the effects of opioids [16]. Naloxone is used to rapidly reverse opioid overdose and ideally prevent death from overdose. Based on our client’s request, our model estimates that naloxone is effective in 50% of its administrations. Naloxone availability appeared to have some of the most meaningful effects on outcome measures. Interestingly, increased availability of naloxone was associated with increased overdoses, but a decreased death rate. We believe that by increasing the probability of receiving naloxone, fewer patients are dying and are remaining in the community. With the increased number of pain patients, the number of overdoses subsequently increases due to the larger sample. This trend seems to also be apparent in both the opioid and the heroin user populations.
PDMP, or Prescription Drug Monitoring Program, is a statewide electronic database which collects designated data on substances dispensed in the state [17]. PDMP is designed to ensure that any individual patient does not receive more than their intended prescription by guarding against prescription “double-dipping”. Our results suggest that PDMP compliance seems to have little effect on outcomes. That said, prior research suggests that increased PDMP compliance has more significant effects over longer simulations such as 20 years in the future [4]. Such a long duration simulation was out of scope for this project, but future research should investigate this claim in the population of Durham.
Emergency departments (ED) may distribute new opioid prescriptions. Smaller initial doses are thought to decrease the rate at which compliant opioid users become dependent on their prescriptions. Our findings suggest that ED initial dosages over 75 MME are associated with increased heroin overdoses and deaths. This finding supports the hypothesis that increased initial doses lead to patients with high tolerance and desire for opioids. This high tolerance and desire may lead compliant opioid users to seek additional narcotics such as heroin, eventually leading to increased heroin overdoses and death.
As previously described, buprenorphine treatment diminishes the effects of physical dependence to opioids, such as withdrawal symptoms and cravings [12]. Buprenorphine can be used in isolation or along with other treatments such as naltrexone. Buprenorphine may have a higher effectiveness compared to other treatments such as naltrexone, and thus higher changes of buprenorphine treatment should be associated with decreased relapse rates in noncompliant opioid and heroin users. However, our results do not suggest that this increased effectiveness has a meaningful impact on outcomes.
Physicians and EDs may distribute new opioid prescriptions. Policies such as the NC STOP Act are aimed at reducing opioid prescriptions in the hopes of decreasing all outcomes [18]. Our findings do not suggest any meaningful effect of prescribing rates on outcomes.
Opioid overdose deaths affect both rural and urban populations in Durham equally. However, opioid overdose deaths do appear to be most prevalent in middle-aged white men. Initial exploratory data analyses allude to potential hotspots for overdoses in areas with public parks or areas adjacent to recovery communities. Further quantitative and qualitative research is needed to validate this hypothesis.
Our results suggest that predicting opioid misuse is far from a simple task. Easily available demographic data alone is not enough to generate accurate opioid misuse predictions; and geographic locations of where drug mortality occurs are not necessarily indicative of where users actually live. Due to this low performance, we were unable to incorporate our predictions into our ABM work. Further research should focus on augmenting demographic data with additional data sources in order to improve accuracy and carry these findings into ABM approaches.
Using ABM, we successfully modeled the outcomes of pain patients in Durham. This step should not be understated, as it required combining an extensive body of research into a single model, a task that was thought by many health officials to be impossible. Our ABM is a meaningful step in understanding the complex behaviors and relationships involved in the lives of local chronic opioid and heroin users. This is proof of concept that these data can be combined to provide meaningful insight, with the understanding that these models are just a starting point, as properly parameterizing them, and ensuring they encompass all major effects, requires significant future work.
From our ABM, we found two major takeaways. First, our estimated probability of overdose is much higher than previous research suggests. Second, our model suggests that almost all heroin overdoses are linked to batches of heroin laced with fentanyl. It is unclear whether these are global phenomena that may affect all opioid users, or if these are a Durham-specific finding. Regardless, future research should examine these results through case studies.
ABM is an ideal approach for modeling complex relationships. We observed that often when heroin user deaths increase so do the number of heroin users. Results like these may seem obvious, but many modeling approaches do not support these types of findings, making ABM an ideal choice for future research.
Our findings suggest that increased naloxone availability and ED initial doses below 75 MME are associated with improved outcomes such as decreased overdoses and death rates. However, interventions such as increased buprenorphine availability and average prescribing rates do not meaningful affect outcomes. This is evidence that policies such as the NC STOP Act may not have their intended effect, or that resulting shifts in behavior may still result in negative outcomes.
The small population of Durham and consequently low number of opioid-related deaths makes accurate estimates for the model parameters even more important. With fewer agents, small tweaks in the model can result in widely different results. ABM approaches may be better suited for larger populations with higher death rates. For instance, Wilkes County, which has a population of approximately 68,000 residents saw 60 opioid deaths between the years of 2013 and 2016, a rate of 88 deaths per 100,000 people over the course of a three year period [9]. Durham, on the other hand, saw 36 deaths between 2013 and 2016, a rate of 12 deaths per 100,000 people in the same time period [9].
Inherent to an ABM approach is the assumption that all entities and relationships remain stable. In other words, an ABM simulation of a five-year period assumes that, over the course of the five years, no additional policies are introduced, all medical facilities remain in operation, and the population remains constant. Unfortunately, this is far from reality. For instance, in Durham, pharmacies were allowed to dispense Naloxone under a 2015 standing order, but widespread limiting of prescribed controlled substances was not active until 2017 with the introduction of the STOP Act [18]. Therefore, not only do these interventions cover different timeframes within a model, but the outcome measures that help us assess the quality of our model were not always available and/or may differ in the way they were recorded 10 years ago versus today. Moreover, we assume that all individuals share similar decision-making processes, which in reality are impacted greatly by individual life circumstances such as culture, socioeconomic status, and life experience. The assumptions associated with ABM are most likely not reflective of reality and should be examined further in future research.
Perhaps the most significant limitation of our analysis is that of the lack of an optimized solution to any ABM calibration. With so many parameters and relationships to adjust, there are seemingly infinite solutions to Durham County outcome calibration, and ours is only one such solution. Due to this limitation, our findings cannot be considered conclusive evidence, but merely suggest areas or further, more definitive research approaches.
A final limitation of our research was the number of model iterations we were able to complete. Even given the small population of Durham, our each ABM iteration used significant computing power and took almost an hour to complete. Additional iterations of each model would increase the accuracy of outcome estimates and thus future research should focus on obtaining additional computing power to run these models. Moreover, additional computing power would also facilitate the exploration of combining multiple interventions and any associated interaction effects. We briefly attempted combining multiple interventions, but additional computing resources would greatly expedite this process.
Additional computational resources would vastly increase the speed of replication and further exploration of this ABM. Specifically in regards to invention effect estimates, increased simulation sample sizes would increase the accuracy of our predictions. Moreover, additional computational power would facilitate additional combinations of model features not yet explored. This is a relatively simple improvement to make that would lead to potentially enormous gains.
We recommend further research and exploration into this application of ABM to modeling the lives and transitions of drug users. Many assumptions were made in the process of this project, each of which could be isolated and examined in detail. The resulting model from our work is one of many possible models that could explain the real-life outcomes we see. Qualitative interviews with key informants are the next best step towards identifying true population measures. Interviews should be pursued with any agent that touches or is impacted by this modeled simulation of drug user lives. Therefore, drug users, families impacted by addiction, pharmacists, providers, health educators, addiction peer sponsors, medical examiners, EMS personnel, ED nurses, and other subject matter experts would all provide valuable insight into the underlying mechanisms of the opioid epidemic in Durham, NC.
One trend we observed was that although increased naloxone availability may lead to fewer deaths, it may also lead to higher rates of non-compliance and more opioid overdoses. A focus group with a group of drug users could explore topics around Naloxone use, and determine if the phenomenon includes cognitive behavioral components, such as a reduced perceived risk of overdose due to the commonly available Naloxone. Further qualitative research is also recommended to explore the hypothesized 1.7 factor increase in probability for opioid overdoses for the Durham population. These are just some examples of nuanced relationships between predictor variables, and interactions that may not be apparent in current models, but may come to light through interviews.
Informational interviews would also provide additional information from professionals who are involved with this crisis in the day to day. For example, interviewing state medical examiners would shed light on overall trends in the circumstances leading to drug overdose deaths, including more specific information on the drugs contributing to death. The State Department of Health and Human Services is well positioned to work with medical examiners, as they are authorized to work with their data. Exploring the extent to which heroin deaths are attributed to fentanyl would determine if the bad batch rates used in our model are in fact the leading cause of more heroin overdose deaths in recent years.
As we have seen in our own work and in trends of the past, public health trends shift. As policies and programs are put in place to address one public health concern, another emerges. The opioid crisis is not immune to this phenomenon. Already, the opioid crisis has shifted from predominantly prescription opioid overdose deaths to heroin deaths; and now there is a rise in overdoses due to cocaine overdoses following tighter regulations on opioids. Future work should examine additional drugs, including cocaine, as we see that regulation of one drug often leads to a shift in overdoses to other drugs. A good extension of this work would have the situational awareness to assess and adjust to emerging public health concerns.
[1] National Institute on Drug Abuse. (2019, January). Opioid Overdose Crisis.
[2] NCDHHS (2019). North Carolina’s Opioid Action Plan.
[3] National Institute on Drug Abuse. (2020, March). Overdose Death Rates.
[4] Bobashev, G., Goree, S., Frank, J., & Zule, W. (2018, July). Pain Town, an Agent-Based Model of Opioid Use Trajectories in a Small Community. In International Conference on Social Computing, Behavioral-Cultural Modeling and Prediction and Behavior Representation in Modeling and Simulation (pp. 274-285). Springer, Cham.
[5] SAMSHA (2019a). Buprenorphine Provider Locator.
[6] NCDHHS Safer Syringe Initiative (2019). Syringe Exchange Programs.
[7] NC Dept of Insurance (2019). Operation Medicine Drop.
[8] SAMHSA (2012). Substance Use and Mental Disorders in the Raleigh-Durham-Cary CSA.The NSDUH Report.
[9] NC DPH IVP Branch (2018). North Carolina Poisoning Surveillance Definitions.
[10] RTI RTI U.S. Synthetic Household Population
[11] SAMSHA (2018). National Survey for Drug Use and Health
[12] SAMSHA (2019b). Buprenorphine.
[13] Johnson, R. E., Jaffe, J. H., & Fudala, P. J. (1992). A controlled trial of buprenorphine treatment for opioid dependence. Jama, 267(20), 2750-2755.
[14] Dunn, K. M., Saunders, K. W., Rutter, C. M., Banta-Green, C. J., Merrill, J. O., Sullivan, M. D., ... & Von Korff, M. (2010). Opioid prescriptions for chronic pain and overdose: a cohort study. Annals of internal medicine, 152(2), 85-92.
[15] Dasgupta, N., Funk, M. J., Proescholdbell, S., Hirsch, A., Ribisl, K. M., & Marshall, S. (2016). Cohort study of the impact of high-dose opioid analgesics on overdose mortality. Pain Medicine, 17(1), 85-98.
[16] National Institute on Drug Abuse. (2020, February). Opioid Overdose Reversal with Naloxone.
[17] US Department of Justice (2016, June). State Prescription Drug Monitoring Programs.
[18] NC Medical Board (2019). Understanding the STOP Act.
An ABM Approach to Addressing the Opioid Crisis: How can we predict the effects of public health intervention on a unique community of pain patients?